Biodata Capitalism, After the Flush: Privacy, Profit, and the Vanishing Biocommons
archive


Public toilet monitoring station in a train station in Shanghai | Photo Credit: Tina Guirguis
Biodata Capitalism, After the Flush: Privacy, Profit, and the Vanishing Biocommons
This article traces how biodata capitalism converts bodily tissues and waste into investible data assets that drive prediction, surveillance, and profit. Following the flush, I map three linked sites where waste becomes value: (1) wastewater surveillance that now monitors everything from viral load to drug consumption at granular scales; (2) household smart toilets that auto-classify stool, quantify biomarkers, and stream intimate metrics to apps; and (3) biobanks and stool banks that standardize donations into clinical inputs for diagnostics and pharmaceutical R&D. While these infrastructures can deliver real public-health gains and new therapeutics, they also rely on unpaid clinical labor, weak privacy protections, and legal-financial arrangements that privatize downstream benefits. Pipelines and business models shift care from the biocommons (“we-medicine”) toward bespoke subscription health (“me-medicine”). I argue that toilets, microbiome home testing kits, and sewers now double as extraction rails, promising safety and personalization even as they normalize population profiling and a move toward neoliberal individualized medicine. The article clarifies the stakes and political economy of microbiome-era infrastructures, showing how everyday sanitation is being rewired for speculative accumulation.
Follow the Flush
Biodata capitalism names a regime in which bodily materials such as tissues, DNA, microbes, and even feces, are converted into data assets for prediction, surveillance, governance, and profit. Our living and excreting bodies become investible datasets that feed bespoke preventive care and downstream pharmaceutical products. Fecal sampling now anchors epidemic research, microbiome mapping, and pharmaceutical development, revaluing waste as a diagnostic tool, medical treatment, and source of data for state surveillance as well as biomedical research and development. Every day infrastructures increasingly double as information gathering machines. The toilet and the sewer now function as interfaces that render bodies and the greater population computationally legible. What follows are some of the implications that surface once we follow the flush.
The Good, the Bad, and the Ugly
Wastewater Surveillance: Improved Health Outcomes, Surveillant Regimes
Wastewater surveillance samples sewage in sewers, septic tanks, and treatment plants to detect biomarkers shed in urine and feces. During COVID-19, viral titers shed in feces in wastewater, offered early epidemiological warnings to help determine the viral loads of neighborhoods, quarantines, and to help allocate resources efficiently (Thompson et al. 2020).
Not only have viruses such as Polio, SARS-CoV-2, COVID-19, and others been monitored through wastewater surveillance, wastewater epidemiology has also been used to detect a wide range of substances, including: cocaine, marijuana, methamphetamines, opioids, ecstasy, artificial sweetener, heroin, ketamine, prescription pharmaceuticals, tobacco, alcohol, and many other substances. The state is able to discreetly monitor a variety of legal and illegal consumption patterns and trends within a community using wastewater-based epidemiology. Several countries have begun integrating such monitoring into national drug detection and enforcement programs. In China, for example, municipal initiatives use sewer analytics to guide policing and interdiction (Du et al. 2015; Cyranoski 2018; Wang et al. 2019; Gao et al. 2020). In the United States, in North Carolina, a robotic wastewater sampling platform was deployed in ten residential manholes to collect hourly samples over a twenty-four period to detect the presence of a custom panel of codeine, buprenorphine, and other opioids in the community’s wastewater (Endo et al, 2020).
Sampling resolution can move from a metropolitan catchment down to a neighborhood, building, or even a single lateral line without the knowledge of those being tracked and with no clear indications of how the information will be used (Thompson et al. 2020).
The public-health upside is real: noninvasive, relatively inexpensive, and responsive, these systems can flag outbreaks, reveal trends that surveys miss, and inform targeted interventions. They also open new streams of value. It is unclear if sewer data can be licensed to public agencies, campus health systems, or private employers. Device and user data from self-analyzing smart toilets inside the home can be bundled into subscription models that sell continuous risk scoring, bespoke advice, and supplements. This is precisely the speculative promise that attracts capital to the sector. Revenues are imagined not only from immediate public-health contracts or device sales, but from derivative products such as algorithms, supplements, and partnerships that can be patented, licensed, and scaled (Cooper 2008; Sunder Rajan and Leonelli 2013).
The same features, however, carry risks. Over-granular wastewater sampling can drift from population health toward community profiling, and longitudinal retention can enable inference about specific sites or households (Thompson et al. 2020). In the domestic setting, smart-toilet data often sits outside strong medical-privacy regimes. Intimate metrics can be routed to marketing partners, health companies, or wellness brokers, in line with profit models that reward continual repurposing and linkage of datasets (Zuboff 2019; Cooper 2008). The result is a widening gray zone where sanitary infrastructures, built in the name of health, double as extraction rails without clear limits on data use, licensing, and privacy.
Biobanks: Free Clinical Labor, Pharmaceutical R&D
Feces carry dense communities of microbes. When a patient’s gut is out of balance, or experiencing dysbiosis, introducing microbes extracted from the feces of a healthy donor can reset the system. That is the premise of fecal microbiota transplantation (FMT). Donors whose good microbes survive screening, freezing, and encapsulation provide material that can rebalance the gut and, by extension, affect immune function, metabolism, and the gut–brain axis with downstream effects on mood and cognition. In this framing, shit is no longer abject; it is extremely biovaluable. A biological fragment that, once isolated, standardized, and routed through lab protocols, becomes knowable, exchangeable, and exploitable.
To scale that promise, institutions have built stool banks, which are biobanks that collect and store feces. OpenBiome is the largest of these stool banks that screens would-be donors (acceptance rates around three percent), pays those who pass roughly $40–$60 per sample, and supplies clinicians with prescreened material for FMT. Donors must produce on schedule, in clinical settings, and under ongoing surveillance; their bodies, habits, and calendars become part of the pipeline. This is clinical labor, the routine low-glamour work by which research subjects provide in vivo and in vitro access to tissue and data. The samples they generate are processed and sold for $595 per treatment or $950 per capsule course. That’s quite a mark-up for human shit. In national biobanks the logic is similar. Participants’ specimens are often linked to health records, fixing them in a productive relationship with research infrastructures across their lives and even posthumously. Samples can be reanalyzed as techniques advance, and data can be bundled with access fees, making the bank itself an economic resource (Mitchell and Waldby 2010).
Once standardized and databased, fecal and other biospecimens feed a chain that runs from academic labs to diagnostics firms, pharmaceutical companies, and investors. Publicly funded discoveries are encouraged to take patent form and then be licensed to private actors, creating revenue streams and investible futures (Cooper 2008). Diagnostics and pharma braid their roadmaps so that tests create customers for therapies, and therapies justify new tests. The result is a market architecture designed to co-produce knowledge and value (Sunder Rajan and Leonelli 2013). In this speculative bioeconomy, each new microbial signature or dysbiosis score can become an asset to market a new subscription regimen, a companion diagnostic, a probiotic formula, or a dataset to be partnered or licensed. These infrastructures expand markets of risk, and create new categories of the potentially sick, growing the demand for testing and prevention.
There are clear benefits. Stool banks expand clinical access and safety, allowing FMT to be delivered more consistently, especially for recurrent C. difficile infection. Large biobanks accelerate discovery by enabling longitudinal studies at scale, pairing specimens with health records helps stratify patients and target trials more precisely. The microbiome turn has opened new therapeutic avenues and diagnostics including risk scorings, probiotic or postbiotic candidates, and potential adjuncts for metabolic, inflammatory, and neuropsychiatric conditions, making personalized and preventive care feel tangible.
Yet the people whose bodies make the system possible have little claim on the value that follows. Donors and participants create the biovalue through ongoing clinical labor, but once a specimen leaves the body, property claims largely vanish. The landmark Moore v. Regents decision held that excised tissue used to create profitable cell lines does not belong to the patient, effectively treating it as abandoned waste in “safe hands.” In practice, standard consent plus de-identification mean no royalties when biospecimens seed lucrative products. Meanwhile, the price of downstream diagnostics or therapeutics often exceeds what contributors can afford. As the microbiome economy expands, households take on more unpaid work through self-sampling at home test kits, logging bodily functions, and adhering to medical protocols, while value accrues upstream to platform owners, patent holders, and investors. This is the contradiction at the heart of biodata capitalism: shit becomes commodity, donors become indispensable workers, and the products of their labor circulate beyond their reach (Mitchell and Waldby 2010; Cooper 2008).
Neoliberal Medicine: A Shift from the Biocommons to Bespoke Healthcare
Classical public health rests on the biocommons—sewers, clean water systems, vaccination campaigns, and other infrastructures built for universal access. Biodata capitalism shifts the center of gravity toward bespoke preventive services through subscriptions, at-home tests, custom probiotics, and insurer-linked wellness programs delivered on proprietary platforms. The biotech industry has seen a proliferation of start-ups focusing on microbiome health via home testing kits as seen in the chart below, which displays just a handful of these ventures.
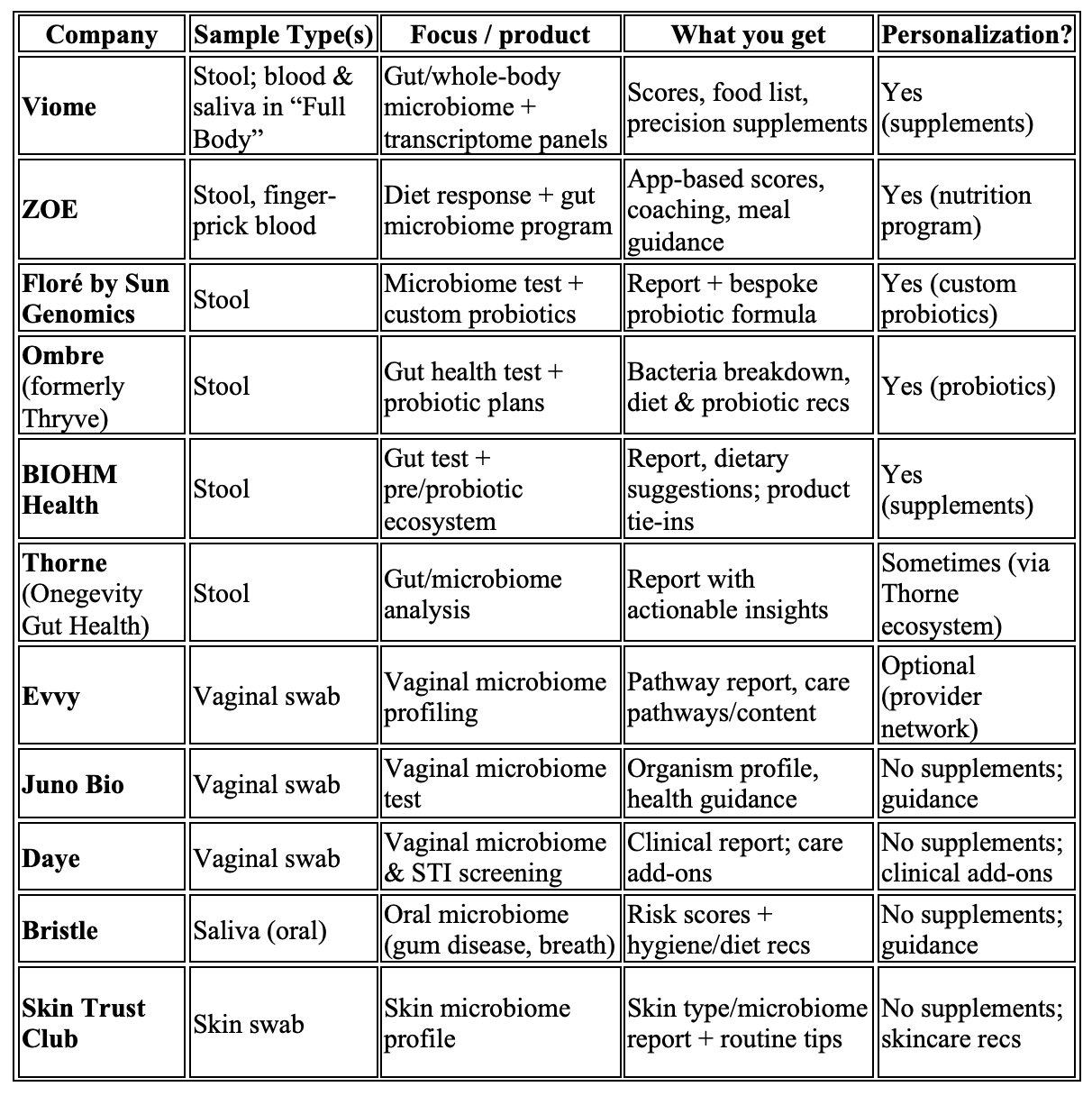
Personalization has genuine benefits. For those with access, tailored recommendations and closer monitoring can improve adherence, catch problems early, and make care feel responsive. Researchers can move faster when they control tests and data, and investors will underwrite risky ventures when exclusive rights promise returns (Cooper 2008). Yet as medical treatments, analytic pipelines, and curated datasets migrate behind paywalls, public systems become tenants in someone else’s infrastructure. Open science and universal provision struggle to keep pace, and rapid, equitable responses are harder to mount when core tools require commercial permission. The political economy narrows from “We-medicine” fostered in the biocommons to “Me-medicine,” (as demonstrated in the chart above), shifting responsibility for health onto individuals and households while value accrues upstream to platform and patent owners (Dickenson 2013).
Conclusion
Wastewater surveillance, biobanks, and fecal testing make the transition toward a neoliberal individualistic form of medicine visible. Profitability is built into the infrastructure. The same toilets and pipes that carry water and waste now carry security and policing surveillance and investible signals. The same kits that promise empowerment over your health feed data inventories. The same banks that invoke solidarity and the future of medical research and development, underpin patents and market exclusivities (Mitchell and Waldby 2010). Industry analyses describe the structural logic as pharmaceutical and diagnostic companies form dozens of partnerships annually, so revenues accrue on both sides of the pipeline (Diaceutics 2017).
Cooper’s account of the biotech–neoliberal alliance clarifies the horizon as biological materials are reorganized as speculative assets, enabling growth “without finite limit” so long as life can be further partitioned, patented, and priced (Cooper 2008). The ethical cost, as access to biospecimens and research tools are privatized, is the risk of a shrinking biocommons, slowly moving toward an anti-commons, where overlapping rights and exclusivities restrict the very resources needed for collective benefit (Dickenson 2013). In short, bespoke microbiome services do not merely sit atop the public health system; they rewire it, redirecting shared infrastructures toward private accumulation while asking the public to supply both the samples and the subscriptions.
Choi, P. M., J. F. O’Brien, and K. V. Thomas. 2018. “Wastewater-Based Epidemiology Biomarkers: Past, Present and Future.” Trends in Analytical Chemistry 105: 453–69.
Cooper, Melinda. 2008. Life as Surplus: Biotechnology and Capitalism in the Neoliberal Era. Seattle: University of Washington Press.
Cyranoski, David. 2018. “China Uses Sewage Surveillance to Target Drug Crime.” Nature 562: 313–14.
Diaceutics. 2017. Pharma–Diagnostic Partnerships Landscape (industry white paper). Belfast: Diaceutics Group.
Dickenson, Donna. 2013. Me Medicine vs. We Medicine: Reclaiming Biotechnology for the Common Good. New York: Columbia University Press.
Du, P., J. Li, J. Zeng, J. Chen, and J. Zhang. 2015. “Monitoring Illicit Drug Use in China by Wastewater Analysis.” Science of the Total Environment 536: 91–98.
Endo, N., S. Ghaffur, J. L. Baker, and D. L. Sedlak. 2020. “High-Frequency Wastewater Sampling for Community-Level Opioid Monitoring.” Environmental Science & Technology 54: 8001–10.
Gao, J., X. Li, Y. Chen, and Y. Wang. 2020. “Wastewater-Based Epidemiology for Illicit Drug Monitoring in Chinese Cities.” Water Research 170: 115–28.
Lai, F. Y., J. O’Brien, et al. 2011. “Refining the Estimation of Illicit Drug Consumption by Wastewater Analysis.” Addiction 106: 1411–22.
Mitchell, Robert, and Catherine Waldby. 2010. “National Biobanks: Clinical Labor, Risk Production, and the Creation of Biovalue.” In Tissue Economies: Blood, Organs, and Cell Lines in Late Capitalism, 107–46. Durham, NC: Duke University Press.
OpenBiome. n.d. “About/FAQs.” Cambridge, MA: OpenBiome.
Sunder Rajan, Kaushik, and Sabina Leonelli. 2013. “Introduction: Biomedical Trans-Actions, Postgenomics, and Knowledge/Value.” Public Culture 25 (3): 463–75.
Thompson, J. R., et al. 2020. “Wastewater Surveillance for SARS-CoV-2 as an Early Warning System.” mSystems 5 (4): e00445-20.
Wang, S., L. Zhang, X. Sun, and J. Li. 2019. “Illicit Drug Consumption Trends Revealed by Wastewater-Based Epidemiology in China.” Environmental Science & Technology 53: 6581–90.
Zuboff, Shoshana. 2019. The Age of Surveillance Capitalism. New York: PublicAffairs.


![MP Materials, which operates this rare-earth open-pit mine in Mountain Pass, California, is one of 10 US companies added to China's export control list [File: Steve Marcus/Reuters]](/sites/default/files/styles/small_square/public/images/2026-01-28T223535Z_178008069_RC2LAJAJ37I6_RTRMADP_3_USA-MINING-TRUMP-PRICE-1770293508.jpg?itok=DDF89Uj9)